 Introduction For this assignment, I have created visual aids to be used to inform Crystal on the importance of monitoring maternal vital signs and abdominal examination in labour. Crystal is hoping for a spontaneous labour and birth with no pharmaceutical pain relief so it is key she sees these comprehensive assessments as guarding, promoting and facilitating her normal physiological process while ensuring safety by identifying complications for her and her baby 1,2. For the visual aids, I have created some affirmation displays with associated information about routine maternal checks that may be offered to Crystal during labour. These designs can be used in several ways:
I have used some of my own feminine and nature-based images that will aim to increase her sense of comfort, relaxation, and well-being. Feminine and nature images have also been shown to lower maternal heart rates, shorten labours, reduce epidural use and increase Apgar scores 3,4 that will support Crystal’s aspirations. I have used a consumer-friendly font and use non-medical language. I have used affirmations taken from the website ‘Healthline’ 5. I see the aid being used as a handout in an antenatal session with some more detailed discussion had with each page/card. The discussion can then be sustained with Crystal using the affirmations within her own home and labour setting. The maternity setting can enhance this association and the environment by using the framed versions in the labour room. Temperature
Heart/Pulse Rate
Respiration Rate
Blood Pressure
Abdominal Palpation
Contraction Palpation
Concluding remarksIt is important when talking to a woman about these clinical checks that often care settings impose time constraints which do not allow for their individual variation of spontaneous labour, but that informed consent will be acknowledged and her autonomy supported 20. To support her autonomy, midwives are required to be with the woman rather than only doing things to her to then become better attuned to her evolving situation and safety. Midwives can integrate these clinical checks into the whole dynamic of care, rather than having them be the central concern 21.
References(1) International Confederation of Midwives [ICM]. Essential Competencies for Midwifery Practice, 2019.
(2) Nursing and Midwifery Board of Australia [NMBA]. Midwife Standards for Practice, 2018. (3) Aburas, R.; Pati, D.; Casanova, R.; Adams, N. G. The Influence of Nature Stimulus in Enhancing the Birth Experience. HERD Health Environ. Res. Des. J. 2017, 10 (2), 81–100. https://doi.org/10.1177/1937586716665581. (4) Setola, N.; Naldi, E.; Cocina, G. G.; Eide, L. B.; Iannuzzi, L.; Daly, D. The Impact of the Physical Environment on Intrapartum Maternity Care: Identification of Eight Crucial Building Spaces. HERD Health Environ. Res. Des. J. 2019, 12(4), 67–98. https://doi.org/10.1177/1937586719826058. (5) Zapata, K. 20 Powerful Birth Affirmations to Encourage and Inspire You. Healthline. https://www.healthline.com/health/pregnancy/birth-affirmations#example-birth-affirmations. (6) Johnson, R.; Taylor, W.; Smith, S. de-Vitry; Bayes, S. Temperature. In Skills for Midwifery Practice Australian & New Zealand Edition; Elsevier Australia, 2022; pp 41–50. (7) National Institute for Health and Care Excellence [NICE]. Intrapartum Care for Healthy Women and Babies. 2017. (8) Safer Care Victoria [SCV]. Care during labour and birth. Safer Care Victoria. https://www.bettersafercare.vic.gov.au/clinical-guidance/maternity/care-during-labour-and-birth (accessed 2022-05-11). (9) Lavesson, T.; Källén, K.; Olofsson, P. Fetal and Maternal Temperatures during Labor and Delivery: A Prospective Descriptive Study. J. Matern. Fetal Neonatal Med. 2018, 31 (12), 1533–1541. https://doi.org/10.1080/14767058.2017.1319928. (10) Schouten, F.; Wolf, H.; Smit, B.; Bekedam, D.; de Vos, R.; Wahlen, I. Maternal Temperature during Labour. BJOG Int. J. Obstet. Gynaecol. 2008, 115 (9), 1131–1137. https://doi.org/10.1111/j.1471-0528.2008.01781.x. (11) Australian College of Midwives. National Midwifery Guidelines for Consultation and Referral, 4th ed.; ACM: Canberra, 2021. (12) Johnson, R.; Taylor, W.; Smith, S. de-Vitry; Bayes, S. Pulse. In Skills for Midwifery Practice Australian & New Zealand Edition; Elsevier Australia, 2022; pp 51–58. (13) Jackson, K.; Anderson, M.; Marshall, J. E. Physiology and Care During the First Stage of Labour. In Myles Textbook for Midwives; Elsevier Limited, 2020; pp 447–499. (14) Towers, C. V.; Trussell, J.; Heidel, R. E.; Chernicky, L.; Howard, B. C. Incidence of Maternal Tachycardia during the Second Stage of Labor: A Prospective Observational Cohort Study. J. Matern. Fetal Neonatal Med. 2019, 32 (10), 1615–1619. https://doi.org/10.1080/14767058.2017.1411476. (15) Johnson, R.; Taylor, W.; Smith, S. de-Vitry; Bayes, S. Respiration. In Skills for Midwifery Practice Australian & New Zealand Edition; Elsevier Australia, 2022; pp 59–68. (16) Blackburn, S. Maternal, Fetal, & Neonatal Physiology: A Clinical Perspective, 5th Edition.; Elsevier Saunders: Maryland Heights, 2016. (17) Johnson, R.; Taylor, W.; Smith, S. de-Vitry; Bayes, S. Blood Pressure. In Skills for Midwifery Practice Australian & New Zealand Edition; Elsevier Australia, 2022; pp 69–90. (18) Johnson, R.; Taylor, W.; Smith, S. de-Vitry; Bayes, S. Abdominal Examination during Labour. In Skills for Midwifery Practice Australian & New Zealand Edition; Elsevier Australia, 2022; pp 309–312. (19) Weckend, M.; Davison, C.; Bayes, S. Physiological Plateaus during Normal Labor and Birth: A Scoping Review of Contemporary Concepts and Definitions. Birth 2022, birt.12607. https://doi.org/10.1111/birt.12607. (20) de Jonge, A.; Dahlen, H.; Downe, S. ‘Watchful Attendance’ during Labour and Birth. Sex. Reprod. Healthc. 2021, 28, 100617. https://doi.org/10.1016/j.srhc.2021.100617. (21) Bradfield, Z.; Hauck, Y.; Duggan, R.; Kelly, M. Midwives’ Perceptions of Being ‘with Woman’: A Phenomenological Study. BMC Pregnancy Childbirth 2019, 19 (1), 363. https://doi.org/10.1186/s12884-019-2548-4.
0 Comments
 This essay will evaluate the influence of environmental and philosophical factors on the normal progress of labour and the midwife’s role in relation to these. In this context the normal progress of labour is defined as the spontaneous onset and advancement of labour and includes the physiological and psychological environments that support effective labour resulting in the vaginal birth of the baby and afterbirth 1. When addressing the influence of environmental and philosophical factors on this normal development it is important to first address the natural interplay of hormones in this process. Labour and birth include neurobiological processes that facilitate the neuroendocrine, psychological, and physiological aspects of parturition 2,3. These systems include oxytocin mediated endogenous pain, fear, and stress relief, which influences the mothers ́ experiences, behaviour and physiology to birth and facilitates their transition to motherhood 2,3. When this process is affected by the adrenalin mediated fight-or-flight reflex, thus increasing stress and anxiety, there is an increase in maternal beta-endorphins to high levels that extend the labour process by influencing this easily modifiable oxytocin system, thereby decreasing the chances of normal birth 3. The presence of undesired persons, brisk procedures, separation from planned known support, bright environment, bothersome noises, time pressure, lack of privacy, practices that impinge upon the labouring woman’s body, and an emphasis on policy rather than individualised response to women’s needs and preferences all increase maternal adrenalin levels 3. Oxytocin is not released in the presence of high levels of adrenaline and it is how this stress, anxiety and fear can change a labouring woman's neurohormonal constitution 3,4. Understanding the profound importance of respecting and promoting this hormonal development is not enough to promote normal birth if the birthing environment does not support normal birth physiology 5,3. The birth environment is a multifaceted concept that includes the physical structures, sensory influences, birth companions, and care provider’s presence and philosophies, as well as psychological spaces of territory, safety, spirituality, and culture 5,6. Much research has been done around the physical birthplace design and its importance in safer maternity care and improved staff experiences 7,8. Aspects of design that have been found to support the natural hormonal cascade of birth include: having access to a bath and shower, private ensuite toilet facilities, adjustable ambient and natural light, and space to move freely with flexible room configurations to enable privacy and avoid feeling exposed 7,4. Setola et al. 7 and Aburas et al. 9 also discuss the use of feminine and nature based artwork and images to increase a sense of comfort, relaxation, and well-being, lower maternal heart rates, shorten labours, reduce epidural use, increase Apgar scores, and screen medical equipment. Jenkinson et al.’s 4 report also includes the positive impact of design features including soft floor furnishings, windows with views of natural landscapes, and access to nature and spaces for relevant traditional ceremonies. Maintaining oxytocin requires a woman to be in a calm, non-threatening and supportive environment that feels private, safe, familiar and undisturbed 3. This sense of security and intimacy is enhanced by being in a space that feels welcoming, comfortable and cosy and offers the choice to personalise 7. It also requires an atmosphere to foster distraction from pain to support this hormone orchestration 7. This form of ambient environment consistently demonstrates lower rates of neonatal admissions, labour augmentation, analgesia use, instrumental and caesarean section births, episiotomies, and active management of the placenta 10,7. Normal labour progress is also enhanced by physical support from labour companions and the birth environment should be accommodating them 7,11. It should be set up to support the midwives with features of friendliness, functionality, and freedom to do their job as guardians for a healthy, normal birth 12. Research shows that labour wards are mainly organised to reduce risks and treat complications and are thus dominated by care focussed on pathology which is important but also hinders and limits the midwife in their role to protect the women’s hormonal safety bubble 10. In this support role, midwives have a presupposition to protect this bubble from disruptions and establish a private, undisturbed atmosphere of familiarity, safety and autonomy 6,10. This can be initiated by establishing the family’s needs and preferences and encouraging them to personalise the space to be more homelike 6,10,13. This could include covering or moving the equipment that emphasises risk, and being recumbent, like the centrality of the bed, and encouraging active, upright positions 8,10. Upright and changing positions are better for the baby; they enhance normal labour and reduce the rate of instrumental birth, episiotomy, and shorten second stage of labour 14. The midwife can facilitate this calm space by adjusting the lighting, reducing unnecessary noise, offering music and aroma-therapy, and providing equipment like birth balls, stools, and other apparatus to promote a physiological labour 5,4. They may offer the stress relief of physical touch or massage, and reassurance that in turn mediates oxytocin release to reduce pain and fear 2,3. It is important to ensure that the birthing woman does not feel observed as it can impact on her sense of privacy 15,16. If the midwife looks relaxed and has a place to sit, the mother feels reassured of their presence and that there are no time constraints to the process 10. The neocortex can also be disrupted by language, therefore, remaining silent and unobtrusive and asking only necessary questions will help maintain a state of hormonal balance 16. Any necessary communication should be sensitive and effective during this intrapartum care 17. Other midwifery roles to maintain this conducive environment include ensuring the room, water, and towels for the baby are an appropriate temperature, providing food and water, partner support and preparation and checking of safety and medical equipment in the space 18. Complementing this care would be the inclusion of continuity of carer 6. The birth environment is also affected by the woman’s relationship with her midwife and the philosophy the midwife has 4. Often this philosophy is hard to differentiate from place of birth 19 but will be independently evaluated as an influence on the normal birth process. Birth philosophy can usually be broken into two main categories: the ‘medical/technocratic model’ and the ‘midwifery/holistic/social model’ 20. Grigg’s 20 medical model is doctor and pathology centred and includes ideas of the body and mind being separate, birth being a hospitalised medical condition, and technology, supervision and intervention being needed to ensure an outcome of a live mother and baby. This model views pain as a problem needing relief, therefore influencing the normal progress of labour, leading the birthing environment to become a ‘surveillance room’ 7. The midwifery model focusses on care being woman centred where midwives are the experts of the normal birth process and includes features of holistic, psychosocial, experiential, and emotional care guarded by observation and focusing not only on a healthy mother and baby but also on birth satisfaction 20. This philosophy of supporting and promoting the physiological process is grounded in the midwifery codes and competencies 11,21,22. It involves ‘working with pain’ as normal and positive 23 and focuses on creating a birthing room that is a ‘sanctum’ 7. The choices and philosophies of women and their partners are influenced by their maternity experiences and knowledge, personal, sociocultural, and political norms, but the major influence is their sense of safety and their belief regarding risk 19,24. There is often a struggle between a desire for a physiological birth, the increasing perceived risk technology can avoid, and the perceived positive experience that technology can offer 5. Women and midwives often choose a birthplace as a protection from or stimulus for their philosophy of childbirth 25. Most women choose to give birth in a hospital setting because it is a good match for what they believe 26, whereas woman with philosophies that seek physiological comfort measures and options such as waterbirth may choose to birth at home 27. Midwife partnerships that involve an individual shared birth philosophy exhibit more sustainability and individual satisfaction, and create fewer communication breakdowns due to tensions and subcultures within the workforce 15,28. This also benefits women who have chosen their midwife or place of birth according to their birth beliefs by ensuring they receive the same philosophical continuity of “care” no matter who attends them 29. Although philosophy of birth may guide principles for behaviour and choices around intrapartum care, it is important to remember that each woman’s birth is individual and care should remain woman-centred 19. This is especially relevant when working with cultural groups who are often stereotyped as having uniform beliefs 30. Women are all cultural beings with varying values and beliefs and yet they are all individuals with their own experiences influenced by class, gender, age, religion and sexual orientation 30. Ultimately women want to give birth to healthy babies in an environment that is clinically and psychologically safe and with care providers who support their philosophical beliefs 11. This essay has evaluated how these aspects of philosophy and environment have the potential to influence the normal progress of labour through the hormonal system. It has addressed how a midwife can respond to these factors in a culturally competent, collaborative and evidence-based way to assess, plan and provide safe psychological and clinical care. References
(1) American College of Nurse-Midwives [ACM]; Midwives Alliance of North America; National Association of Certified Professional Midwives [NMBA]. Supporting Healthy and Normal Physiologic Childbirth: A Consensus Statement by ACNM, MANA, and NACPM. J. Perinat. Educ. 2013, 22 (1), 14–18. https://doi.org/10.1891/1058-1243.22.1.14. (2) Olza, I.; Uvnas-Moberg, K.; Ekström-Bergström, A.; Leahy-Warren, P.; Karlsdottir, S. I.; Nieuwenhuijze, M.; Villarmea, S.; Hadjigeorgiou, E.; Kazmierczak, M.; Spyridou, A.; Buckley, S. Birth as a Neuro-Psycho-Social Event: An Integrative Model of Maternal Experiences and Their Relation to Neurohormonal Events during Childbirth. PLOS ONE2020, 15 (7), e0230992. https://doi.org/10.1371/journal.pone.0230992. (3) Buckley, S. J. Hormonal Physiology of Childbearing: Evidence and Implications for Women, Babies, and Maternity Care. Childbirth Connect. Programs Natl. Partnersh. Women Fam. 2015. (4) Jenkinson, B.; Josey, N.; Kruski, S. BirthSpace: An Evidence-Based Guide to Birth Environment Design; Queensland Centre for Mothers & Babies, The University of Queensland: The University of Queensland, 2013. (5) Stark, M. A.; Remynse, M.; Zwelling, E. Importance of the Birth Environment to Support Physiologic Birth. J. Obstet. Gynecol. Neonatal Nurs. 2016, 45 (2), 285–294. https://doi.org/10.1016/j.jogn.2015.12.008. (6) Carlsson, I.-M.; Larsson, I.; Jormfeldt, H. Place and Space in Relation to Childbirth: A Critical Interpretive Synthesis. Int. J. Qual. Stud. Health Well-Being 2020, 15 (sup1), 1667143. https://doi.org/10.1080/17482631.2019.1667143. (7) Setola, N.; Naldi, E.; Cocina, G. G.; Eide, L. B.; Iannuzzi, L.; Daly, D. The Impact of the Physical Environment on Intrapartum Maternity Care: Identification of Eight Crucial Building Spaces. HERD Health Environ. Res. Des. J. 2019, 12(4), 67–98. https://doi.org/10.1177/1937586719826058. (8) Townsend, B.; Fenwick, J.; Thomson, V.; Foureur, M. The Birth Bed: A Qualitative Study on the Views of Midwives Regarding the Use of the Bed in the Birth Space. Women Birth 2016, 29 (1), 80–84. https://doi.org/10.1016/j.wombi.2015.08.009. (9) Aburas, R.; Pati, D.; Casanova, R.; Adams, N. G. The Influence of Nature Stimulus in Enhancing the Birth Experience. HERD Health Environ. Res. Des. J. 2017, 10 (2), 81–100. https://doi.org/10.1177/1937586716665581. (10) Andrén, A.; Begley, C.; Dahlberg, H.; Berg, M. The Birthing Room and Its Influence on the Promotion of a Normal Physiological Childbirth - a Qualitative Interview Study with Midwives in Sweden. Int. J. Qual. Stud. Health Well-Being2021, 16 (1), 1939937. https://doi.org/10.1080/17482631.2021.1939937. (11) World Health Organisation [WHO]. WHO Recommendations: Intrapartum Care for a Positive Childbirth Experience; World Health Organisation [WHO]: Geneva, 2018. (12) Hammond, A.; Homer, C. S. E.; Foureur, M. Friendliness, Functionality and Freedom: Design Characteristics That Support Midwifery Practice in the Hospital Setting. Midwifery 2017, 50, 133–138. https://doi.org/10.1016/j.midw.2017.03.025. (13) National Institute for Health and Care Excellence [NICE]. Intrapartum Care for Healthy Women and Babies. 2017. (14) Zang, Y.; Lu, H.; Zhang, H.; Huang, J.; Zhao, Y.; Ren, L. Benefits and Risks of Upright Positions during the Second Stage of Labour: An Overview of Systematic Reviews. Int. J. Nurs. Stud. 2021, 114, 103812. https://doi.org/10.1016/j.ijnurstu.2020.103812. (15) Davis, D. L.; Homer, C. S. E. Birthplace as the Midwife’s Work Place: How Does Place of Birth Impact on Midwives? Women Birth 2016, 29 (5), 407–415. https://doi.org/10.1016/j.wombi.2016.02.004. (16) Odent, M. Odent M: Birth Territory: The Besieged Territory of the Obstetrician. In Fahy K, Foureur M, and Hastie C (Eds): Birth Territory and Midwifery Guardianship. Oxf. Elsevier 2008, 131. (17) Malesela, J. M. L. Midwives Perceptions: Birth Unit Environment and the Implementation of Best Intrapartum Care Practices. Women Birth 2021, 34 (1), 48–55. https://doi.org/10.1016/j.wombi.2020.04.003. (18) Thorpe, J.; Anderson, J. Supporting Women in Labour and Birth - Midwifery Preparation for Practice. In Midwifery Preparation for Practice; Pairman, S., Tracy, S. K., Dahlen, H. G., Dixon, L., Eds.; 2019; pp 504–531. (19) Tracy, S.; Grigg, C. Birthplace and Birth Space - Midwifery Preparation for Practice. In Midwifery Preparation for Practice; Pairman, S., Tracy, S. K., Dahlen, H. G., Dixon, L., Eds.; 2019; pp 89–112. (20) Grigg, C.; Tracy, S. K.; Daellenbach, R.; Kensington, M.; Schmied, V. An Exploration of Influences on Women’s Birthplace Decision-Making in New Zealand: A Mixed Methods Prospective Cohort within the Evaluating Maternity Units Study. BMC Pregnancy Childbirth 2014, 14 (1), 210. https://doi.org/10.1186/1471-2393-14-210. (21) International Confederation of Midwives [ICM]. Essential Competencies for Midwifery Practice, 2019. (22) Nursing and Midwifery Board of Australia [NMBA]. Midwife Standards for Practice, 2018. (23) Leap, N. Working with Pain in Labour. New Dig. 2010, No. 49, 22–26. (24) Downe, S.; Finlayson, K.; Oladapo, O.; Bonet, M.; Gülmezoglu, A. M. What Matters to Women during Childbirth: A Systematic Qualitative Review. PLOS ONE 2018, 13 (4), e0194906. https://doi.org/10.1371/journal.pone.0194906. (25) Dahlen, H. G.; Downe, S.; Jackson, M.; Priddis, H.; de Jonge, A.; Schmied, V. An Ethnographic Study of the Interaction between Philosophy of Childbirth and Place of Birth. Women Birth 2020, S1871519220303656. https://doi.org/10.1016/j.wombi.2020.10.008. (26) Declercq, E. R.; Sakala, C.; Corry, M. P.; Applebaum, S.; Herrlich, A. Report of the Third National U.S. Survey of Women’s Childbearing Experiences. 2013, 94. (27) Maude, R.; Caplice, S. Using Water for Labour and Birth - Midwifery Preparation for Practice. In Midwifery Preparation for Practice; Pairman, S., Tracy, S. K., Dahlen, H. G., Dixon, L., Eds.; 2019; pp 281–295. (28) Catling, C. J.; Reid, F.; Hunter, B. Australian Midwives’ Experiences of Their Workplace Culture. Women Birth2017, 30 (2), 137–145. https://doi.org/10.1016/j.wombi.2016.10.001. (29) Gilkison, A.; Hewitt, L. Supporting Midwives, Supporting Each Other - Midwifery Preparation for Practice. In Midwifery Preparation for Practice; Pairman, S., Tracy, S. K., Dahlen, H. G., Dixon, L., Eds.; 2019; pp 281–295. (30) Hartz, D.; Sherwood, J. Midwives Working with Aboriginal and Torres Strait Islander Women - Midwifery Preparation for Practice. In Midwifery Preparation for Practice; Pairman, S., Tracy, S. K., Dahlen, H. G., Dixon, L., Eds.; 2019; pp 158–174. 11/2/2021 0 Comments Pre-existing Mental Illness May has presented to her first antenatal hospital visit at 20 weeks gestation with a self-acknowledged mental illness. In this essay I will discuss mental illness and its impact on attachment and maternal and child outcomes. Midwifery care provided during the perinatal period will be discussed with reference to contemporary literature. Risk and protective factors will be considered, as well as screening, medication use, and consultation and referral in care. The ongoing care of May will be addressed including planning to promote positive maternal bonding and infant attachment in this potentially at-risk situation. Globally, the rates for perinatal mental illness range from 10 to 41 per cent dependent on both definition and measurement1. In Australia, suicide is a leading cause of maternal death, categorised as ‘aggravated by the physiologic effects of pregnancy’ 2. These effects can occur in the perinatal period as an ongoing, aggravation or relapse of an existing condition, or as a new response to the changes in the perinatal period 1 and show worse outcomes for women, children and families living with these conditions 3. Outcomes include higher rates of pre-eclampsia 4 and other poor obstetric consequences 5, low weight and preterm birth for the neonate 6, and are further compounded by the biophysical changes, social upheavals and adjustments in the postnatal period 7,8. Mental illness may impair the woman’s ability to bond and care for her infant during pregnancy and in the early postpartum period 5, impacting the ability of the infant to form a secure attachment 9,10. Without this security, the infant’s ongoing development is compromised 11. The deficits in the rapidly developing neurology of the child impair physical, psychological, language, emotional and behavioural growth and impact the immune function with effects continuing into adulthood 5,12. Later in life we find this childhood stress has been associated with a broad range of health problems such as increased reactivity to trauma, cognitive deficits, and psychiatric and behavioural disorders 13. This highlights the importance of woman-centred, mental health education, assessment, support and treatment for the perinatal period, especially when more women are beginning their pregnancies or developing these issues during their pre and post-natal periods 3. In the present case study, May has disclosed an existing mental health illness. The midwife is in a privileged position to care for and respond to May’s emotional state and to offer support and referrals 14. This is within the midwife’s scope of practice, respecting their professional relationship and in a culturally safe, trauma-informed manner 15. The first step is to understand May’s situation and personal, risk and protective factors that can make her and her baby more vulnerable or resilient 11. These factors can be identified through routine ‘booking visit’ checks that include psychosocial, medical, and physical assessment, history-taking, through empathetic and non-judgemental listening 16,4, and a mental state examination 17. Risk factors to look for include May’s personal and family history 11, low socioeconomic status, membership of minority groups, substance misuse, low support resources, poor self-esteem 11, current and past trauma 1, and intimate partner and family violence 18. As May’s number of risk factors increase, so too does the likelihood of her poorer psychosocial health 11. Of particular note for May, the major risk factor for developing a perinatal mental health condition is a pre-existing mental health history 11,19,4. Her illness could range from managing a normal life through to feeling disabled, chronically symptomatic and on medication, and should therefore be addressed in relation to her particular case 16. The midwife should enquire if May is currently in contact with psychiatric services or if they need to be engaged. Fear of judgment by health professionals can lead women suffering mental illness to delay their first consultation 11. This is another risk factor for May. It is also important to notice any resilience factors where May is able to adapt well to adversity, facilitating better psychological strength, and coping behaviours 1. These strengths can include knowledge, skills, attitude, self-efficacy 11 and partner, family, and social support 20. The Edinburgh Postnatal Depression Scale (EPDS) is used as a screening tool and would be offered to May as a screening instrument 21. The midwife should repeat this screening at least once later in pregnancy or if clinically indicated 11. An appropriately translated version should be used if applicable, such as if May identifies as an Aboriginal and/or Torres Strait Islander 21. If assessing for psychosocial risk, administer the Antenatal (Psychosocial) Risk Questionnaire as well 4. Before screening and assessment, the midwife should ensure May’s privacy and that only appropriate persons are present 21. Health professionals should be available to provide advice, supervision, support and follow-up to deal with potential responses and issues raised 4. May should be provided with a clear explanation of the purpose of the screening and the limits to confidentiality before offering her informed consent 4. Screening is supported by collaboration, consultation and referral pathways that involve working with mental health and other obstetrics services 1. Collaboration with members of May’s health care team needs to be coordinated between all professionals ensuring continuity of care 22. This involves effective sharing of information and documentation between all involved, including May 14. Building on collaboration, consultation includes other professionals with specialised knowledge 22. This could be indicated by concerns for a current or historical psychological or perinatal mental health issue, an EPDS score greater than 12, a positive response to the EPDS self-harm question (Q10), antenatal depression and/or anxiety, significant social isolation and lack of social support 22. If the level of responsibility required for May falls outside the midwife’s scope of practice, a referral is needed and the primary responsibility transferred to another qualified health service professional or provider, while the midwife still remains a key member of May’s team and maintains continuity of care 22. This should be planned early enough in the pregnancy that May can build trusting relationships as a safety net for her and her baby 4. Referral includes for an acute and unstable mental health concern 16. If May is using medication for her mental illness, the midwife should have knowledge and understanding of the use of common psychiatric drugs in pregnancy and lactation 16. Most antidepressants are not associated with major congenital abnormalities, with preferred drugs being Sertraline and Citalopram 23. Mental health medications to avoid include Clomipramine, Paroxetine and Sodium Valproate 24. Modifying the use of psychotropic medications during pregnancy, like ceasing Lithium with bipolar disorder, can be detrimental to both maternal and infant outcomes 24. Consultation with a specialist pharmacist is important to provide access to their expertise in medication management 24. The midwife should discuss all possible support and treatment options and their potential problems and advantages 23, facilitating choice so that May maintains control 16. This information should be based on evidence and promote emotional health 14. Ongoing care with May should involve opportunities for her to discuss her expectations and experiences including any issues and concerns that may have arisen 4. The midwife should monitor for signs of relapse, especially if medication is modified before or during pregnancy 4. Providing realistic expectations of motherhood and the post-natal period, including the normal hormonal, psychological, emotional and physical changes, will promote greater wellbeing for May, maximising her coping skills, self-regulation and bonding with her infant 25. Exploring strategies May has previously used and reinforcing these strengths to help develop parental confidence could avoid or minimise factors that contribute to a traumatic birth 26. Working with May to increase her capacity to manage her own problems in the future 27 could reduce stress by promoting autonomy 16. If the midwife is reliable, accessible and provides a secure base for May, this could create a safe space for May to be a secure base for her child and will enhance her reflective capacity, emotional regulation and empathy 28. This will promote positive attachment in the next generation 29. I have provided evidence of the significance of the midwife in offering woman-centred, continuity of care planning for May who is at risk of adverse perinatal mental health outcomes. I have looked at the importance of maternal bonding and infant attachment for the future healthy development of the child and provided risk and resilience factors of relevance and the pathway of screening, consulting and referring for May to build a collaborative multidisciplinary team to support and promote the current and future wellbeing for her and her baby. By non-judgementally and empathetically working within their scope of practice, the midwife has the capacity to change transgenerational mental health patterning for May. References(1) Jomeen, J.; Fleming, S. E.; Martin, C. R. Women with a Diagnosed Mental Health Problem. In Psychosocial Resilience and Risk in the Perinatal Period; Thomson, G., Schmied, V., Eds.; Routledge: Abingdon, Oxon ; New York, NY : Routledge, 2017., 2017; pp 9–26. https://doi.org/10.4324/9781315656854-2.
(2) Australian Institute of Health and Welfare. Maternal Deaths in Australia. 2019. https://doi.org/10.25816/7Q4E-G697. (3) CCOPMM; Safer Care Victoria. Victoria’s Mother, Babies and Children - 2019; 58; Victorian Government: Melbourne, Victoria, Austraia, 2021; p 57. (4) Department of Health. Clinical Practice Guidelines: Pregnancy Care; Australian Government Department of Health: Canberra, 2018. (5) McNamara, J.; Townsend, M. L.; Herbert, J. S. A Systemic Review of Maternal Wellbeing and Its Relationship with Maternal Fetal Attachment and Early Postpartum Bonding. PLOS ONE 2019, 14 (7), e0220032. https://doi.org/10.1371/journal.pone.0220032. (6) Eastwood, J.; Ogbo, F. A.; Hendry, A.; Noble, J.; Page, A.; Group, E. Y. R. The Impact of Antenatal Depression on Perinatal Outcomes in Australian Women. PLOS ONE 2017, 16. (7) Osman, N. N.; Bahri, A. I. Impact of Altered Hormonal and Neurochemical Levels on Depression Symptoms in Women During Pregnancy and Postpartum Period. 2019, 9. (8) Rihua, X.; Haiyan, X.; Krewski, D.; Guoping, H. Plasma Concentrations of Neurotransmitters and Postpartum Depression. 2017, 8. (9) 1st 1001 Days APPG. Building Great Britons. Conception to Age 2; First 1001 Days All Parties Parliamentary Group: London, 2015. (10) Bowlby, J. Attachment Theory and Its Therapeutic Implications. Ann. Am. Soc. Adolesc. Psychiatry 1978, No. 6, 5–33. (11) Schmied, V.; Dixon, L. Women’s Psychosocial Health and Wellbeing. In Midwifery : preparation for practice; Elsevier Australia: Chatswood, NSW, 2019; p 23. (12) Biaggi, A.; Conroy, S.; Pawlby, S.; Pariante, C. M. Identifying the Women at Risk of Antenatal Anxiety and Depression: A Systematic Review. J. Affect. Disord. 2016, 191, 62–77. https://doi.org/10.1016/j.jad.2015.11.014. (13) Provençal, N.; Binder, E. B. The Effects of Early Life Stress on the Epigenome: From the Womb to Adulthood and Even Before. Exp. Neurol. 2015, 268, 10–20. https://doi.org/10.1016/j.expneurol.2014.09.001. (14) COAG Health Council. Woman-Centred Care: Strategic Directions for Australian Maternity Services. Department of Health August 2019. (15) NMBA. Code of Conduct for Midwives. Nursing and Midwifery Board of Australia. 2018. (16) Raynor, M. D.; Mason, A.; Williams, M.; Wallroth, P.; Skene, G.; Whibley, S. Perinatal Mental Health. In Myles Textbook for Midwives (Seventeenth Edition); 2020; pp 756–784. (17) Hercelinskyj, G.; Alexander, L. Asseessment and Diagnosis. In Mental health nursing; ProQuest Ebook Central, 2019. (18) Zhang, S.; Wang, L.; Yang, T.; Chen, L.; Qiu, X.; Wang, T.; Chen, L.; Zhao, L.; Ye, Z.; Zheng, Z.; Qin, J. Maternal Violence Experiences and Risk of Postpartum Depression: A Meta-Analysis of Cohort Studies. Eur. Psychiatry 2019, 55, 90–101. https://doi.org/10.1016/j.eurpsy.2018.10.005. (19) Cao, H.; Zhou, N.; Leerkes, E. M.; Qu, J. Multiple Domains of New Mothers’ Adaptation: Interrelations and Roots in Childhood Maternal Nonsupportive Emotion Socialization. J. Fam. Psychol. 2018, 32 (5), 575–587. https://doi.org/10.1037/fam0000416. (20) Abdollahpour, S.; Keramat, A. The Relationship between Perceived Social Support from Family and Postpartum Empowerment with Maternal Wellbeing in the Postpartum Period. J. Midwifery Reprod. Health 2016, 4 (4). https://doi.org/10.22038/jmrh.2016.7612. (21) Austin, M.-P.; Highet, N.; Expert Working Group. Mental Health Care in the Perinatal Period: Australian Clinical Practice Guideline; Centre of Perinatal Excellence.: Melbourne, 2017; p 121. (22) Australian College of Midwives. National Midwifery Guidelines for Consultation and Referral, 4th ed.; ACM: Canberra, 2021. (23) Molenaar, N. M.; Kamperman, A. M.; Boyce, P.; Bergink, V. Guidelines on Treatment of Perinatal Depression with Antidepressants: An International Review. Aust. N. Z. J. Psychiatry 2018, 52 (4), 320–327. https://doi.org/10.1177/0004867418762057. (24) Niethe, M.; Whitfield, K. Psychotropic Medication Use during Pregnancy. J. Pharm. Pract. Res. 2018, 48 (4), 384–391. https://doi.org/10.1002/jppr.1483. (25) Rizzo, I.; Watsford, C. The Relationship between Disconfirmed Expectations of Motherhood, Depression, and Mother–Infant Attachment in the Postnatal Period. Aust. Psychol. 2020, 55 (6), 686–699. https://doi.org/10.1111/ap.12472. (26) Hollander, M. H.; van Hastenberg, E.; van Dillen, J.; van Pampus, M. G.; de Miranda, E.; Stramrood, C. A. I. Preventing Traumatic Childbirth Experiences: 2192 Women’s Perceptions and Views. Arch. Womens Ment. Health 2017, 20 (4), 515–523. https://doi.org/10.1007/s00737-017-0729-6. (27) NMBA. Midwife Standards for Practice. Nursing and Midwifery Board of Australia. October 1, 2018. (28) Berry, K.; Danquah, A. Attachment-Informed Therapy for Adults: Towards a Unifying Perspective on Practice. Psychol. Psychother. Theory Res. Pract. 2016, 89 (1), 15–32. https://doi.org/10.1111/papt.12063. (29) Newman, L.; Sivaratnam, C.; Komiti, A. Attachment and Early Brain Development – Neuroprotective Interventions in Infant–Caregiver Therapy. Transl. Dev. Psychiatry 2015, 3 (1), 28647. https://doi.org/10.3402/tdp.v3.28647.  All women experience emotional changes in relation to being a new parent. Pregnancy and birth are considered significant events that create physiological and behavioural adaptive responses known as emotions 1. There are often unexpected reactions of sadness, self-doubt, guilt, disempowerment, trauma, and loneliness 2,3. This essay will firstly describe how normal bodily changes that result from childbirth may affect the emotional wellbeing of the woman as she makes this transition. It will then use current literature to articulate the midwife’s role in caring for the woman’s psychological health at this time, paying particular attention to evidence on the midwife’s scope of practice, assessment of care needed, normal and abnormal expectations in the postnatal period, including health promotion, and increased risk factors. Lastly, this essay will describe some community resources that the midwife may offer the family to address any queries, concerns, and referral pathways that are needed. Anatomically a woman’s body changes in pregnancy and childbirth due to the physical changes of the physiological birth process 4. This includes significant breast changes, uterine involution and the body returning towards a pre-pregnant state 4. Depending on her perspectives about body image, these may affect her emotional wellbeing during her transition to parenthood 5,6. Hormonal puerperium changes have an effect on emotional states, namely the decreases in oestrogen and progesterone and an increase in prolactin and oxytocin 4. Changes in neurotransmitters such as serotonin, dopamine and norepinephrine also play a significant role in psychosocial and depressive behaviours 4,7,8. Within the midwife’s scope of practice, midwives care for and respond to a woman’s emotional state and offer access to needed support 9,10. Some evidence argues that this is an area midwives need to pay more attention to 11, haveing the potential to create an environment that may buffer the negative effects of obstetric complications post birth 12–14. Successful parental transitions have been attributed to the midwife’s ability to connect to women 15 and offer non-judgemental family focussed, consistent care that empowers women 16 built on a relationship of trust and understanding 17. How women are cared for by health professionals impacts how early parenthood is managed and emotional support is vital 18. This relationship is enhanced with continuity of care and being home-based where the woman feels safe, receives more quality time, experiences greater confidence, and a sense of community and cultural acceptance 11,19–21. When this level of support is achieved it strengthens the woman’s self-efficacy, her ability to organise support, and instigate constructive coping strategies 15. When assessing and prioritising the emotional care that may be provided to the post-natal woman, the midwife should ask the woman herself at each contact about her health and concerns 22. These are often called ‘listening visits’ 23. This may involve allowing a woman to debrief and share her birth experience 13,22,24. Some new mothers feel negatively towards their birth experience with emotions influenced by hormonal fluctuations, fear, depression and violations during labour 25. Others feel empowered, confident and more relaxed about their labour and birth experience 25. Listening involves tuning into the woman’s emotional state, and midwives are in the perfect position to screen for any issues 22,26. Creating these positive experiences should not exclude provision of honest information 27. The information a midwife offers should be based on evidence and promote emotional health appropriate to that family 9,10,28,29. This includes ensuring the woman is sufficiently informed and reassured about the realistic expectations of the post-natal period 15,24,27. They should inform the family of the new demands of parenthood, including increased mood-disorder and sometimes depression which diminishes self-regulation 30. Woman tend to emotionally regulate to their baby’s distress, their own sleep deprivation, any breastfeeding challenges, and the new family dynamics, so it is therefore important that these situations are anticipated 30. It is also recommended that there is discussion about the devalued postpartum body and the emotional expectations about ‘bouncing back’ 31. The woman should be informed that between three to seven days postpartum, she may experience what is known as ‘baby blues’ 4. She should be informed that this is a normal transient physiological stage where the adjusting hormones are said to cause tearfulness, mood changes, irritability, forgetfulness, fatigue and some minor stress and anxiety in 50% of mothers 4. Families should also be educated to watch for abnormal signs of continuing emotional disturbances that escalate to post-natal depression (PND) and postpartum psychosis 4. These affect 10% and 3% respectively and include exacerbated sleep and anxiety symptoms as well as reduced self-esteem and weight loss which may escalate to delusions and hallucinations 4. Included in a midwife’s emotional health promotion of the post-natal period should be some recommendations for a range of supports for this transition as pharmacological and psychotherapeutic therapies may not offer complete solutions 32. Partner, family and social support has a positive impact on maternal wellbeing and reduces depression and anxiety 2 24. So too does religion, infant bonding, forming friendships, education, and utilising childcare 33. It has also been shown that exercise can increase positive feelings 34 and singing to babies can strengthen emotional thoughts towards them 32. When addressing the emotional care a midwife may provide a post-natal woman and her family, we cannot ignore that one in three women experience post-traumatic stress (PTS) following giving birth 12,13. This may have been brought about by obstetric violence, including spoken humiliation, ignored needs and wishes, invasive or forced medical procedures or interventions, an unwell baby, previous life events, pregnancy trauma and concerns around babies wellbeing 18,25. For 1.7-9% of women, this can develop into post-traumatic stress disorder (PTSD) where there is intense or prolonged psychological distress 35. Both PTS and PTSD symptoms lead to poor maternal health, infant bonding and family relations 35, and should be treated with heightened awareness, extra consistent, non-dismissive, supportive, emotional care to reduce early parenting difficulties 18. Time should be allowed for reflection and validation 18 and a referral should be made if appropriate 22. Current literature also shows other risk factors for poor mental health that include a caesarean birth 4,18,35,36, pre-existing emotional experiences 4,18,30,35, an unwanted pregnancy 2, separation from family and culture 33, birth complications, low income 4,27, relationship issues, poor social and emotional support, and the death of baby 4. Particular attention would need to be considered in these situations when a midwife is assessing the level and content of care to provide. Some helpful community resources that a midwife could suggest would be to consult the woman’s General Practitioner with any issues or questions but to also inform her that Victoria has a free Maternal and Child Health (MCH) Service that is focused on the health outcomes for children and families including maternal emotional factors 3. A visit from an MCH nurse is scheduled in their home within two weeks of birth and in-clinic support is offered until the child is school age. The MCH service is guided by the ‘Perinatal mental health and psychosocial assessment’ 37 and includes using the Edinburgh Postnatal Depression Scale (EPDS) screening tool. This tool is used to improve the detection of postnatal depression and is part of the COPE best practice guidelines. The Centre of Perinatal Excellence (COPE) is a national not-for-profit organisation focused on reducing the effects of emotional and mental health problems in the perinatal periods. Their website is easy to navigate and includes many areas of evidence-based support for women and families. COPE have been working with governments and professional bodies since they transitioned from Beyond Blue in 2013. Beyond Blue focuses on anxiety and depression but in a much broader context. They have specific pregnancy and postnatal information and checks. Perinatal Anxiety and Depression Australia (PANDA) is a more specific organisation supporting recovery from perinatal anxiety and depression for individuals and families. Many of the organisations have ‘hotlines’ and have been listed in the resource list Appendix A. In conclusion, when reviewing the literature, we can see that not only do normal physiological changes affect the emotional wellbeing of the woman as she makes this transition to motherhood, but that there are many other factors that need to be considered within a midwife’s scope of practice to offer evidence-based support. This essay covered the assessment needed for care and the normal and abnormal expectations in the postpartum period. It included health promotion solutions and some of the increased risk factors for psychological illness. Lastly, it described some community resources that the midwife may offer the family to address any queries, concerns, and referral pathways that may be needed. References (1) James, W. II.—WHAT IS AN EMOTION ? Mind 1884, os-IX (34), 188–205. https://doi.org/10.1093/mind/os-IX.34.188. (2) Abdollahpour, S.; Keramat, A. The Relationship between Perceived Social Support from Family and Postpartum Empowerment with Maternal Wellbeing in the Postpartum Period. J. Midwifery Reprod. Health 2016, 4 (4). https://doi.org/10.22038/jmrh.2016.7612. (3) Sanders, R.; Lehmann, J.; Gardner, F. Parents’ Experiences of Victoria’s Maternal and Child Health Service during the Transition to Parenthood. Aust. J. Child Fam. Health Nurs. 2018, 15 (1), 9–16. (4) Rankin, J. Puerperium—the Mother. In Physiology in childbearing e-book : With anatomy and related bioscience; Elsevier Health Sciences, 2017; pp 592–595. (5) Prinds, C. Yummy Mummy — The Ideal of Not Looking like a Mother. Women Birth 2020, 8. (6) Rodgers, R. F. A Biopsychosocial Model of Body Image, Disordered Eating, and Breastfeeding among Postpartum Women. 2018, 6. (7) Osman, N. N.; Bahri, A. I. Impact of Altered Hormonal and Neurochemical Levels on Depression Symptoms in Women During Pregnancy and Postpartum Period. 2019, 9. (8) Rihua, X.; Haiyan, X.; Krewski, D.; Guoping, H. Plasma Concentrations of Neurotransmitters and Postpartum Depression. 2017, 8. (9) International Confederation of Midwives. International Code of Ethics for Midwives https://www.internationalmidwives.org/assets/files/general-files/2019/10/eng-international-code-of-ethics-for-midwives.pdf. (10) COAG Health Council. Woman-Centred Care: Strategic Directions for Australian Maternity Services. Department of Health August 2019. (11) Fenwick, J.; Butt, J.; Dhaliwal, S.; Hauck, Y.; Schmied, V. Western Australian Women’s Perceptions of the Style and Quality of Midwifery Postnatal Care in Hospital and at Home. Women Birth 2010, 23 (1), 10–21. https://doi.org/10.1016/j.wombi.2009.06.001. (12) Baptie, G.; Andrade, J.; Bacon, A. M.; Norman, A. Birth Trauma: The Mediating Effects of Perceived Support. Br. J. Midwifery 2020, 28 (10), 724–730. https://doi.org/10.12968/bjom.2020.28.10.724. (13) Baxter, J. Postnatal Debriefing: Women’s Need to Talk after Birth. Br. J. Midwifery 2019, 27 (9), 563–571. (14) Deninotti, J.; Denis, A.; Berdoulat, É. Emergency C-Section, Maternal Satisfaction and Emotion Regulation Strategies: Effects on PTSD and Postpartum Depression Symptoms. J. Reprod. Infant Psychol. 2020, 38 (4), 421–435. https://doi.org/10.1080/02646838.2020.1793308. (15) Walker, S. B.; Rossi, D. M.; Sander, T. M. Women’s Successful Transition to Motherhood during the Early Postnatal Period: A Qualitative Systematic Review of Postnatal and Midwifery Home Care Literature. Midwifery 2019, 79, 102552. https://doi.org/10.1016/j.midw.2019.102552. (16) Wiklund, I.; Wiklund, J.; Pettersson, V.; Boström, A.-M. New Parents’ Experience of Information and Sense of Security Related to Postnatal Care: A Systematic Review. Sex. Reprod. Healthc. 2018, 17, 35–42. https://doi.org/10.1016/j.srhc.2018.06.001. (17) Woodward, B. M.; Zadoroznyj, M.; Benoit, C. Beyond Birth: Women’s Concerns about Post-Birth Care in an Australian Urban Community. Women Birth 2016, 29 (2), 153–159. https://doi.org/10.1016/j.wombi.2015.09.006. (18) Priddis, H. S.; Keedle, H.; Dahlen, H. The Perfect Storm of Trauma: The Experiences of Women Who Have Experienced Birth Trauma and Subsequently Accessed Residential Parenting Services in Australia. Women Birth 2018, 31(1), 17–24. https://doi.org/10.1016/j.wombi.2017.06.007. (19) Cummins, A.; Griew, K.; Devonport, C.; Ebbett, W.; Catling, C.; Baird, K. Exploring the Value and Acceptability of an Antenatal and Postnatal Midwifery Continuity of Care Model to Women and Midwives, Using the Quality Maternal Newborn Care Framework. Women Birth 2021, S187151922100041X. https://doi.org/10.1016/j.wombi.2021.03.006. (20) Forster, D. A.; McKay, H.; Davey, M.-A.; Small, R.; Cullinane, F.; Newton, M.; Powell, R.; McLachlan, H. L. Women’s Views and Experiences of Publicly-Funded Homebirth Programs in Victoria, Australia: A Cross-Sectional Survey. Women Birth 2019, 32 (3), 221–230. https://doi.org/10.1016/j.wombi.2018.07.019. (21) Forster, D. A.; McLachlan, H. L.; Davey, M.-A.; Biro, M. A.; Farrell, T.; Gold, L.; Flood, M.; Shafiei, T.; Waldenström, U. Continuity of Care by a Primary Midwife (Caseload Midwifery) Increases Women’s Satisfaction with Antenatal, Intrapartum and Postpartum Care: Results from the COSMOS Randomised Controlled Trial. BMC Pregnancy Childbirth 2016, 16 (1), 28. https://doi.org/10.1186/s12884-016-0798-y. (22) NICE; RCOG. Postnatal Care NICE Guideline. National Institute for Health and Care Excellence April 20, 2021. (23) Lowenhoff, C.; Appleton, J. V.; Davison-Fischer, J.; Pike, N. NICE Guideline for Antenatal and Postnatal Mental Health: The Health Visitor Role. J. Health Visit. 2017, 5 (6), 290–298. https://doi.org/10.12968/johv.2017.5.6.290. (24) Slomian, J.; Emonts, P.; Vigneron, L.; Acconcia, A.; Glowacz, F.; Reginster, J. Y.; Oumourgh, M.; Bruyère, O. Identifying Maternal Needs Following Childbirth: A Qualitative Study among Mothers, Fathers and Professionals. BMC Pregnancy Childbirth 2017, 17 (1), 213. https://doi.org/10.1186/s12884-017-1398-1. (25) Khajehei, M.; Doherty, M. Women’s Experience of Their Sexual Function during Pregnancy and after Childbirth: A Qualitative Survey. Br. J. Midwifery 2018, 26 (5), 318–328. (26) Moss, K. M.; Reilly, N.; Dobson, A. J.; Loxton, D.; Tooth, L.; Mishra, G. D. How Rates of Perinatal Mental Health Screening in Australia Have Changed over Time and Which Women Are Missing Out. Aust. N. Z. J. Public Health2020, 44 (4), 301–306. https://doi.org/10.1111/1753-6405.12999. (27) Rizzo, I.; Watsford, C. The Relationship between Disconfirmed Expectations of Motherhood, Depression, and Mother–Infant Attachment in the Postnatal Period. Aust. Psychol. 2020, 55 (6), 686–699. https://doi.org/10.1111/ap.12472. (28) NMBA. Code of Conduct for Midwives. Nursing and Midwifery Board of Australia. 2018. (29) NMBA. Midwife Standards for Practice. Nursing and Midwifery Board of Australia. October 1, 2018. (30) Cao, H.; Zhou, N.; Leerkes, E. M.; Qu, J. Multiple Domains of New Mothers’ Adaptation: Interrelations and Roots in Childhood Maternal Nonsupportive Emotion Socialization. J. Fam. Psychol. 2018, 32 (5), 575–587. https://doi.org/10.1037/fam0000416. (31) Johnson, S. “I See My Section Scar like a Battle Scar”: The Ongoing Embodied Subjectivity of Maternity. Fem. Psychol. 2018, 28 (4), 470–487. https://doi.org/10.1177/0959353518769920. (32) Fancourt, D.; Perkins, R. Associations between Singing to Babies and Symptoms of Postnatal Depression, Wellbeing, Self-Esteem and Mother-Infant Bond. Public Health 2017, 145, 149–152. https://doi.org/10.1016/j.puhe.2017.01.016. (33) Russo, A.; Lewis, B.; Joyce, A.; Crockett, B.; Luchters, S. A Qualitative Exploration of the Emotional Wellbeing and Support Needs of New Mothers from Afghanistan Living in Melbourne, Australia. BMC Pregnancy Childbirth 2015, 15 (1), 197. https://doi.org/10.1186/s12884-015-0631-z. (34) Hutt, R. L.; Moore, G. A.; Mammen, M. A.; Symons Downs, D. Postpartum Mothers’ Leisure-Time Exercise Behavior Is Linked to Positive Emotion During Partner Discussions. Res. Q. Exerc. Sport 2017, 88 (4), 447–454. https://doi.org/10.1080/02701367.2017.1375450. (35) Simpson, M.; Schmied, V.; Dickson, C.; Dahlen, H. G. Postnatal Post-Traumatic Stress: An Integrative Review. Women Birth 2018, 31 (5), 367–379. https://doi.org/10.1016/j.wombi.2017.12.003. (36) Alderdice, F. Psychosocial Factors That Mediate the Association between Mode of Birth and Maternal Postnatal Adjustment: Findings from a Population-Based Survey. 2019, 13. (37) Victoria State Government. Perinatal Mental Health and Psychosocial Assessment. Victorian Government 2019. Appendix A
Emotional Wellbeing Resources Pregnancy and Post-Natal COPE - https://www.cope.org.au/ PANDA – 1300 726 306 - https://www.panda.org.au/ General Beyond Blue – 1300 22 4636 - https://www.beyondblue.org.au/ SANE Australia - 1800 18 7263 MindSpot Clinic - 1800 61 44 4/28/2021 0 Comments Racism toward Aboriginal and Torres Strait Islander people within my future midwifery workplace In this essay I will discuss the impact on individuals of implied racism, overt racism and racial commentary toward Aboriginal and Torres Strait Islander people within my future midwifery workplace. I will discuss the differences and offer specific examples and evidence to support the discussion. In the given example, Adam Goodes, an Australian Rules footballer, in 2013 was publicly discriminated against for his features which brought about much commentary and discussion about the normalisation of overt and implied racism and how this gets responded to. Racism is an assumption of natural hierarchy of culturally and characteristically identifiable groups bringing with it bias and prejudice 1. The ‘lesser’ groups are avoidably and unfairly treated differently 2. Within Australia, these groups are protected by the Racial Discrimination Act of 1975 3 and when the football fan publicly labelled Adam an ‘ape’, this violated this act. This public name calling can be categorised as overt or explicit racism where the discriminatory behaviour is clear, conscious, direct, obvious, undisguised and blatant and can manifest in physical violence, unfair treatment and insults 4. Overt racism can intentionally be self-monitored to consciously avoid appearing racist 5. This form of racism has also been called ‘old fashioned’ 6 but over time, legal sanctions have inadvertently created a more subtle form of ‘modern’, implied, implicit, racism that is much harder to detect, label and therefore call out 2. This more covert racism can be found where individuals or organisations behave on the basis of prejudice and stereotypes automatically, unintentionally and unconsciously 7,8. This implied racism can be seen in the relentless ‘booing’ of Mr Goodes, from many different football clubs until his retirement. This reaction appearing outside of normal fan barracking and jeering behaviour. There is an underlying acceptance of discrimination against this man’s heritage and a lack of acknowledgement of the historical cultural oppression. This ‘booing;’ and the responses in the media and social media in responses to the acts of racism are called racial commentary and have the ability to exacerbate any discrimination but also magnify the need for reform. Racism also remains very active across the health sector and midwifery workplace 9 with over 70% of surveyed midwives admitting that some staff were disrespectful and racist to indigenous colleagues in their workplace including stereotyping, discrimination and prejudice 10. Ninety nine percent also agreed that racism negatively impacted student outcomes for First Peoples 10. Indigenous midwifes are feeling unsafe and burnt out and not remaining in the workforce 11. There is also evidence of implicit racism that has influenced hiring decisions in the sector 12. As consumers of health services, First Peoples carry the weight of health inequality 13 and often report experiencing racism 10. Racism causes health inequities and contributes to poor health outcomes experienced by these people 2. Within maternity care, over half of women who identified as Aboriginal, professed experiencing discrimination within their care setting and did not receive care to match their needs 14. These women were more likely to have poor infant health outcomes, including low birthweight and small for gestational age 14. Examples of this implied racism can be brought about by carer anxiety about working with clients who appear different and include not looking at the women, shortening the consultation or withholding information they would otherwise provide 2. When questioned if they ask all clients if they are an Aboriginal or Torres Strait Islander, midwives replied with “Not if they don’t look it.”, “don’t want to offend someone.” 9. This implies that it is shameful to be Aboriginal. Not only is this racism seen on an individual level, but there is also outcome disparity within Australian hospitals affected by institutional racism with an organisational change failure rate of 70% 15. On this level we also see a lack of access to care 9 including Aboriginal women not having the ability to honour customs like birthing on country due to lack of an appropriate insurance product to allow midwives to provide evidence based midwifery continuity of care in this setting 16. Practicing culturally unsafe is racist 2. This includes not listening to or treating a person with dignity and disrespecting their cultural identity 17. Culturally safe maternity care includes an holistic view of a woman’s needs including culture and seeks to reduce any power that may be felt by the women in their care 16. It is important that “only the woman and/or her family can determine whether or not care is culturally safe and respectful” 18 I have defined and discussed the impact on First Nations of implied and overt racism and how racial commentary can affect its effects. I have examined these concepts more comprehensively within my future midwifery workplace, offering specific examples and evidence to support the discussion. As a student and future midwife, I can make a positive contribution to health equity particularly for indigenous Australians by providing care that is culturally safe and respectful. References
(1) Hampton, R.; Toombs, M. Racism, Colonisation/Colonialism and Impacts on Indigenous People. In Indigenous Australians and Health : The Wombat in the Room; Oxford University Press, 2013; p 21. (2) Taylor, K.; Thompson Guerin, P. Determinants of Health. In Health Care and Indigenous Australians : Cultural Safety in Practice : Cultural Safety in Practice; Macmillan Education UK, 2019. (3) Australian Government. Racial Discrimination Act 1975. (4) Lui, P. P. Racial Microaggression, Overt Discrimination, and Distress: (In)Direct Associations With Psychological Adjustment. Couns. Psychol. 2020, 48 (4), 551–582. https://doi.org/10.1177/0011000020901714. (5) Banks, A. J.; Hicks, H. M. Fear and Implicit Racism: Whites’ Support for Voter ID Laws: Fear and Implicit Racism. Polit. Psychol. 2016, 37 (5), 641–658. https://doi.org/10.1111/pops.12292. (6) Pedersen, A.; Beven, J.; Walker, I.; Griffiths, B. Attitudes toward Indigenous Australians: The Role of Empathy and Guilt. J. Community Appl. Soc. Psychol. 2004, 14 (4), 233–249. https://doi.org/10.1002/casp.771. (7) Brownstein, M. Implicit Bias https://plato.stanford.edu/archives/fall2019/entries/implicit-bias/. (8) Quigley, A.; Hutton, J.; Phillips, G.; Dreise, D.; Mason, T.; Garvey, G.; Paradies, Y. Review Article: Implicit Bias towards Aboriginal and Torres Strait Islander Patients within Australian Emergency Departments. Emerg. Med. Australas.2021, 33 (1), 9–18. https://doi.org/10.1111/1742-6723.13691. (9) Sherwood, J.; Mohamed, J. Racism a Social Determinant of Indigenous Health: Yarning About Cultural Safety and Cultural Competence Strategies to Improve Indigenous Health. In Cultural Competence and the Higher Education Sector; Frawley, J., Russell, G., Sherwood, J., Eds.; Springer Singapore: Singapore, 2020; pp 159–174. https://doi.org/10.1007/978-981-15-5362-2_9. (10) Fleming, T.; Creedy, D. K.; West, R. Evaluating Awareness of Cultural Safety in the Australian Midwifery Workforce: A Snapshot. Women Birth 2019, 32 (6), 549–557. https://doi.org/10.1016/j.wombi.2018.11.001. (11) Lai, G.; Taylor, E.; Haigh, M.; Thompson, S. Factors Affecting the Retention of Indigenous Australians in the Health Workforce: A Systematic Review. Int. J. Environ. Res. Public. Health 2018, 15 (5), 914. https://doi.org/10.3390/ijerph15050914. (12) Ditonto, T. M.; Lau, R. R.; Sears, D. O. AMPing Racial Attitudes: Comparing the Power of Explicit and Implicit Racism Measures in 2008: Comparing 2008 Racism Measures. Polit. Psychol. 2013, 34 (4), 487–510. https://doi.org/10.1111/pops.12013. (13) CATSINaM; NMBA. NMBA and CATSINaM Joint Statement on Culturally Safe Care. 2018. (14) Brown, S. J.; Gartland, D.; Weetra, D.; Leane, C.; Francis, T.; Mitchell, A.; Glover, K. Health Care Experiences and Birth Outcomes: Results of an Aboriginal Birth Cohort. Women Birth 2019, 32 (5), 404–411. https://doi.org/10.1016/j.wombi.2019.05.015. (15) Bourke, C. J.; Marrie, H.; Marrie, A. Transforming Institutional Racism at an Australian Hospital. Aust. Health Rev. 2019, 43 (6), 611. https://doi.org/10.1071/AH18062. (16) Kildea, S.; Gao, Y.; Hickey, S.; Nelson, C.; Kruske, S.; Carson, A.; Currie, J.; Reynolds, M.; Wilson, K.; Watego, K.; Costello, J.; Roe, Y. Effect of a Birthing on Country Service Redesign on Maternal and Neonatal Health Outcomes for First Nations Australians: A Prospective, Non-Randomised, Interventional Trial. Lancet Glob. Health 2021, S2214109X21000619. https://doi.org/10.1016/S2214-109X(21)00061-9. (17) Williams, R. Cultural Safety - What Does It Mean for Our Work Practice? Aust. N. Z. J. Public Health 1999, 23(2), 213–214. https://doi.org/10.1111/j.1467-842X.1999.tb01240.x. (18) Nursing and Midwifery Board of Australia. Code of Conduct for Midwives. Nursing and Midwifery Board of Australia. 2018. 2/20/2021 1 Comment Gender Inequality and Birth TraumaFollow on from '1/9/2021 - LOCAL AND GLOBAL BIRTH TRAUMA AND UN SDG#5'  The United Nation’s (UN’s) Sustainable Development Goal 1 of achieving gender equality and empowering all women and girls is an important goal to focus on in my future midwifery profession as the disparities in maternity care are still to be resolved. In this essay I will identify the challenges to the common good in these disparities. I will then discuss the solutions I feel most relevant to help achieve this goal. I will describe how proposed solutions contribute to the realisation of the common good and what the barriers may be in achieving them.
Gender equality means that women and girls enjoy the same rights, resources, opportunities and protections as men and boys. This is important when addressing the common good of a local and global community. Common good is when the inherent human dignity of each individual within that group is acknowledged and is able to flourish to its full potential 2. It also acknowledges that ‘all human beings are born free and equal in dignity and rights ‘ 3. This includes how woman are treated in childbirth. Woman who have been mistreated in their birth process suffer short and long-term physical and psychological health problems 4. These can have an effect on the infant and future child 5 and affect their capacity to thrive and be an active participant in their community. When the common good and therefore gender equality are realised, we will see safer, healthier populations 6. Women will birth feeling empowered to make informed, autonomous choices and will be supported through those choices and whatever outcome follows. This is an ideal situation applicable to the local and global maternal environment. Anecdotal evidence from my local community of public hospitals in Melbourne reflects that women’s birthing processes are far from this ideal. The research tells us that post-traumatic stress rates are as high as 9% for post-natal women 7 and suicide is the third highest cause of maternal deaths in Australia 8. Globally, evidence of the rate of acquiescence and subsequent mistreatment of women in maternity care settings is as high as 40% 9,10. Those joining the midwifery profession have many ways as individuals and groups to address these poor outcomes. We are front-line providers with substantial reach and have the direct capability to help achieve and sustain the UN’s gender equality development goal 11. I will propose three of these solutions within the local and global environment. The first is working within a midwifery-led, continuity of care (COC) model and ensuring that woman have access to woman-centred care. This model is where the midwife is the primary carer from the initial maternity appointment, up to six weeks post-partum 12. Within this model a trust relationship can be established, and midwives can offer person specific knowledge, empowering women to make informed, autonomous choices about their care. Women who participate in COC have better healthcare outcomes and higher satisfaction rates 12,13. The partnering relationship empowers women and is endorsed by the International Confederation of Midwives and the Nursing and Midwifery Board of Australia 14,15. Even with the positive research results concerning this model of supporting woman, it is still only experienced by a very few. Care providers are becoming more specialised and therefore women are more likely to receive fragmented care from different carers 16. This form of fragmented care can be a barrier to establishing a safe, trusting environment where women feel equal and empowered to disclose their thoughts and choices around their care 17. My second proposal addresses barriers to achieving gender equity in our health system. Decisions relating to women’s care should be facilitated with the inclusion of the community it directly relates to. This is referred to as ‘subsidiarity’ and involves the participation and willingness of people to contribute to the consultation process, while keeping in mind the principle of the common good 18. Involvement may include advisory groups within professional employment, joining and being active with the Australian College of Midwives, offering time to projects with the International Confederation of midwives and getting involved with non-government organisations like Human Rights in Childbirth. It is imperative to increase the involvement of midwives in policy and decision-making forums on an institutional, national and international level 11. By being a part of larger organisations, we can advocate for health care policy development, planning, and funding that promotes human rights in childbirth and supports gender equity in places where decisions are made. This advocacy gives a voice to those who often do not have the capacity to be heard in a particular setting 19. A third solution is community engagement. This is an action or process to build relationships with the intention of benefitting the values of a community or group brought together by location, interest, circumstances or vision 20. We can come together as a global family to care for the common good by generating a strong sense of solidarity and connection to offer women a louder voice to address the disparities of those whose rights are extremely compromised. This leads to improved outcomes for communities 21 and stimulates greater international collaboration to attain the UN’s Social Development Goals. Professionals are also able to acquire new skills through mutual learning to bring back to their home environments 11. There are many maternity care engagements internationally to be involved in, particularly in third world countries where resources are lacking, and where women are often not receiving the needed treatment. These engagements may be ‘on the ground’ clinical support, but we can also utilise our own networks to advocate for these people and promote their needs and procurement of resources to improve women’s chances of flourishing within these populations. Some organisations I have become involved in include Birth For Humankind (Melbourne), Birth Time: the documentary (Australia), Loas Birthwork (Loas) and Bumi Sehat (Indonesia). Barriers to involvement in decision making and community engagement groups may include accessibility issues by way of location, skills, resources or language. Realising and agreeing on what constitutes the common good may also be a challenge when many ideas are shared in the community, but ‘free societies do not stay free without the involvement of their citizens’ 22. We can however be open to these challenges and create good conditions for relationship, participation, and community 22. In summary I have examined the gender equity issues for women in my future midwifery profession in my local and the global community. I have addressed how realising the common good is related to achieving the UN’s Sustainable Development Goal of achieving gender equity and empowering all women and girls. I have proposed ways that my professional community can contribute to achieving these goals by working in and advocating for continuity of care models, participating in decision making groups and engaging in community to improve outcomes. As a global midwifery community, we are brought together by focusing on the UN’s goals, but through individual connection to the woman we are working with, we can make these aspirations grow, one woman and baby at a time. References (1) United Nations. Goal 5: Achieve gender equality and empower all women and girls https://www.undp.org/content/undp/en/home/sustainable-development-goals/goal-5-gender-equality.html (accessed Jan 10, 2020). (2) Part Three: Life in Christ https://www.vatican.va/archive/ccc_css/archive/catechism/p3s1c2a2.htm (accessed Jan 28, 2021). (3) United Nations. Universal Declaration of Human Rights https://www.un.org/en/universal-declaration-human-rights/index.html (accessed Aug 29, 2020). (4) Curtin, M.; Savage, E.; Leahy‐Warren, P. Humanisation in Pregnancy and Childbirth: A Concept Analysis. J. Clin. Nurs. 2020, 29 (9–10), 1744–1757. https://doi.org/10.1111/jocn.15152. (5) Anderson, C. A. The Trauma of Birth. Health Care Women Int. 2017, 38 (10), 999–1010. https://doi.org/10.1080/07399332.2017.1363208. (6) The benefits of gender equality https://www.vic.gov.au/benefits-gender-equality (accessed Jan 9, 2021). (7) Simpson, M.; Schmied, V.; Dickson, C.; Dahlen, H. G. Postnatal Post-Traumatic Stress: An Integrative Review. Women Birth 2018, 31 (5), 367–379. https://doi.org/10.1016/j.wombi.2017.12.003. (8) Australian Institute of Health and Welfare. Maternal Deaths in Australia. 2019. https://doi.org/10.25816/7Q4E-G697. (9) Bohren, M. A.; Mehrtash, H.; Fawole, B.; Maung, T. M.; Balde, M. D.; Maya, E.; Thwin, S. S.; Aderoba, A. K.; Vogel, J. P.; Irinyenikan, T. A.; Adeyanju, A. O.; Mon, N. O.; Adu-Bonsaffoh, K.; Landoulsi, S.; Guure, C.; Adanu, R.; Diallo, B. A.; Gülmezoglu, A. M.; Soumah, A.-M.; Sall, A. O.; Tunçalp, Ö. How Women Are Treated during Facility-Based Childbirth in Four Countries: A Cross-Sectional Study with Labour Observations and Community-Based Surveys. The Lancet 2019, 394 (10210), 1750–1763. https://doi.org/10.1016/S0140-6736(19)31992-0. (10) Betron, M. L.; McClair, T. L.; Currie, S.; Banerjee, J. Expanding the Agenda for Addressing Mistreatment in Maternity Care: A Mapping Review and Gender Analysis. Reprod. Health 2018, 15 (1), 143. https://doi.org/10.1186/s12978-018-0584-6. (11) Rosa, W. E.; Kurth, A. E.; Sullivan-Marx, E.; Shamian, J.; Shaw, H. K.; Wilson, L. L.; Crisp, N. Nursing and Midwifery Advocacy to Lead the United Nations Sustainable Development Agenda. Nurs. Outlook 2019, 67 (6), 628–641. https://doi.org/10.1016/j.outlook.2019.06.013. (12) Sandall, J.; Soltani, H.; Gates, S.; Shennan, A.; Devane, D. Midwife-Led Continuity Models versus Other Models of Care for Childbearing Women. Cochrane Database Syst. Rev. 2016. https://doi.org/10.1002/14651858.CD004667.pub5. (13) Jeffers, H.; Baker, M. Continuity of Care: Still Important in Modern-Day General Practice. Br. J. Gen. Pract. 2016, 66 (649), 396–397. https://doi.org/10.3399/bjgp16X686185. (14) International Confederation of Midwives. International Code of Ethics for Midwives https://www.internationalmidwives.org/assets/files/general-files/2019/10/eng-international-code-of-ethics-for-midwives.pdf. (15) Nursing and Midwifery Board of Australia. Code of Conduct for Midwives. Nursing and Midwifery Board of Australia. 2018. (16) Jairath, N.; Donley, R.; Shelton, D.; McMullen, P.; Grandjean, C. Nursing and the Common Good. Soc. Justice Cathol. Health Care 2006, November-December 2006, 59–63. (17) Viveiros, C. J.; Darling, E. K. Barriers and Facilitators of Accessing Perinatal Mental Health Services: The Perspectives of Women Receiving Continuity of Care Midwifery. Midwifery 2018, 65, 8–15. https://doi.org/10.1016/j.midw.2018.06.018. (18) Carter, D. What is Subsidiarity? https://leocontent.acu.edu.au/file/5097fe6c-c77e-4787-bfe9-bf98714d060d/21/UNCC100Refresher.html (accessed Jan 28, 2021). (19) UNCC300 Module 3: Principles of Advocacy. Australian Catholic University 2018. (20) Moore, T.; McDonald, M.; McHugh-Dillon, H.; West, S. Community Engagement: A Key Strategy for Improving Outcomes for Australian Families. 2016, 39, 25. (21) Burton, P.; Goodlad, R.; Croft, J. How Would We Know What Works?: Context and Complexity in the Evaluation of Community Involvement. Evaluation 2006, 12 (3), 294–312. https://doi.org/10.1177/1356389006069136. (22) Mortensen, J. N.; Bech, E. M.; Godrim, F. The Engaged Human: You Are Free for Community. In The Common Good : An Introduction to Personalism; Vernon Press, 2017; pp 57–79.  As a current birth worker and future midwife, I am appalled at the way women are treated in childbirth. The human dignity of this gender in this context seems to be falling short of the United Nation’s (UN’s) Sustainable Development Goal of achieving gender equity and empowering all women and girls. Birth trauma rates are high and the effects on humanity are continually being realised. The UN’s fifth of seventeen Sustainable Development Goals 1 aims to end gender discrimination, violence and harmful practices, seeking to increase compensation, participation, subsidiarity and solidarity. It aims to strengthen reproductive, economic and technological rights and enforceable legislation for all women, girls and the common good. The common good is where all members of a community, by virtue of their innate common humanity, can thrive more easily. Acknowledging that gender inequity most commonly disadvantages females calls for extra focus to be placed on the dignity and empowerment of this group. This will ensure that all in the community are remembered and able to reach their full potential 2,3. Achieving this common good involves modest sacrifices. This could be adjusting the way women are addressed and treated during the epic journey of childbirth. Within maternity units in Melbourne, I see that these measures do not always accomplish these goals. My local community consists predominantly of publicly funded, high level, teaching hospitals. Within their complicated hierarchy of doctors, midwives and birthing women, there is a strong sense of “power over” dominance 4. Working with families, I witness women struggling to gain autonomy over their bodies and babies. I hear stories of disrespect, abuse and subsequent trauma related to their experience. A woman’s birth trauma may involve threatened or actual intense fear, helplessness and loss of control during labour and birth, with the perception of her dignity being stripped 5. Dr Amali Lokugamage at the Royal College of Obstetrician and Gynaecologists World Congress takes this treatment a step further and describes this lack of authority and autonomy as "Obstetric Violence" 6. This form of trauma occurs in birthing settings across the globe. In third world countries, up to 40% of women experience mistreatment in childbirth 7. Women were expected to “obey” rules or else cruelty was deemed justifiable 8. A global analysis showed patterns of normalisation of mistreatment, a "be chaste, be quiet" attitude, woman’s lack of voice about their choices, and insufficient education, rights and resources 9. The global birthing community may vary greatly and can include anything from traditional midwives to highly educated medical specialists. Venues may include dirt floor huts or clinically sterile rooms. Birthing women may be malnourished or affluently healthy and have various levels of understanding, but human dignity in birth can be maintained in any of these situations 10. So why is reducing birth trauma for women important for the common good of the whole community? How mothers feel post birth influences the physiological maternal-infant bonding that occurs 5. This has an effect on breastfeeding, infant behaviour and psychosocial stability 5. Later social development for that child may also be affected 5. Maternally, birth trauma is related to the long-term mental health problems 10 and affects their capacity to flourish and be an active participant in the community. When looking at the broader picture of women’s equity in the local community, we see the influence of women’s active participation. The Victorian government reports that economic productivity and business profitability would increase with more women in the workforce and in leadership. It states that establishing gender equity creates safer and healthier communities. It also recognises that the best way to prevent violence against women is to promote gender equity 11. Globally, the recent reports on the status of the UN’s goal shows reductions in childhood marriage, down 5%, and female genital mutilation, slightly down to 200 million. There has been an increase of 2.6% in the number of women in parliament, 3% in management and positive progress in sexual and reproductive health decision making and education. But these changes are not enough. There is still a lot to be done to achieve gender equity and women’s empowerment in order to attain human rights for everyone 3. I have discussed women’s gender equity issues in my local and the global community. Within my current and future professions, I would like to see some changes made. I would like to witness birth trauma rates at justifiable levels. I would like to see women treated with human dignity in childbirth. I would like to see the UN’s Sustainable Development Goal of achieving gender equity—empowering all women and girls—realised and our local and global population flourishing. References
(1) United Nations. Goal 5: Achieve gender equality and empower all women and girls https://www.undp.org/content/undp/en/home/sustainable-development-goals/goal-5-gender-equality.html (accessed Jan 10, 2020). (2) Manuel Velasquez; Claire Andre; Thomas Shanks; S. J. Meyer; Michael J Meyer. The Common Good. (3) UNFPA. Frequently asked questions about gender equality https://www.unfpa.org/resources/frequently-asked-questions-about-gender-equality (accessed Jan 8, 2021). (4) Dempsey, R. Birth Rights and the Hidden Threat of Obstetric Violence. Crikey.com.au. March 8, 2018. (5) Anderson, C. A. The Trauma of Birth. Health Care Women Int. 2017, 38 (10), 999–1010. https://doi.org/10.1080/07399332.2017.1363208. (6) Lokugamage, A. Royal College of Obstetricians and Gynecologists 2014 World Congress, 2014. (7) Bohren, M. A.; Mehrtash, H.; Fawole, B.; Maung, T. M.; Balde, M. D.; Maya, E.; Thwin, S. S.; Aderoba, A. K.; Vogel, J. P.; Irinyenikan, T. A.; Adeyanju, A. O.; Mon, N. O.; Adu-Bonsaffoh, K.; Landoulsi, S.; Guure, C.; Adanu, R.; Diallo, B. A.; Gülmezoglu, A. M.; Soumah, A.-M.; Sall, A. O.; Tunçalp, Ö. How Women Are Treated during Facility-Based Childbirth in Four Countries: A Cross-Sectional Study with Labour Observations and Community-Based Surveys. The Lancet 2019, 394 (10210), 1750–1763. https://doi.org/10.1016/S0140-6736(19)31992-0. (8) Maung, T. M.; Show, K. L.; Mon, N. O.; Tunçalp, Ö.; Aye, N. S.; Soe, Y. Y.; Bohren, M. A. A Qualitative Study on Acceptability of the Mistreatment of Women during Childbirth in Myanmar. Reprod. Health 2020, 17 (1), 56. https://doi.org/10.1186/s12978-020-0907-2. (9) Betron, M. L.; McClair, T. L.; Currie, S.; Banerjee, J. Expanding the Agenda for Addressing Mistreatment in Maternity Care: A Mapping Review and Gender Analysis. Reprod. Health 2018, 15 (1), 143. https://doi.org/10.1186/s12978-018-0584-6. (10) Curtin, M.; Savage, E.; Leahy‐Warren, P. Humanisation in Pregnancy and Childbirth: A Concept Analysis. J. Clin. Nurs. 2020, 29 (9–10), 1744–1757. https://doi.org/10.1111/jocn.15152. (11) The benefits of gender equality https://www.vic.gov.au/benefits-gender-equality (accessed Jan 9, 2021). As well as the oral presentation we presented a health promotion flyer and website about Anti-D.
9/7/2020 0 Comments An ARGUMENT against mandatory reporting of child abuse against a pregnant woman misusing illicit drugs & alcohol In recent years there have been fewer Australians drinking but an increased use in illicit drugs such as cannabis (+1.2%), cocaine (+1,7%) and ecstasy (+0.8%) 1. Misuse is defined as the use of these substances outside of medical prescription or law 2. When it is evident that a pregnant woman is misusing illicit drugs or alcohol, the enforcement of mandatory reporting for child abuse can seem appropriate. It is important that health care professionals (HCPs) are able to evaluate this in an ethical framework 3 to ensure their responses are based on benefit to the sick and the promotion of health and life. In this essay I will argue that enforcing mandatory reporting is not the correct course of action and in fact would create more harm than potential benefit. I will address the counter arguments and base my thesis on Beauchamp and Childress’s 3 principles of autonomy, justice, beneficence and non-maleficence. This will be done by examining the pregnant woman’s rights, where the duty of carers lies and what some of the potential outcomes may be for the mother, her foetus, her future child and the greater community. It is extremely hard to get accurate statistics about alcohol and drug use in pregnancy due to screening and diagnosis issues 4. However there is research to show that 25% of Australian babies born to mothers who consumed alcohol during pregnancy were diagnosed with fetal alcohol spectrum disorder (FASD) 5. Moreover it is estimated 10-20% of pregnant women in the USA exposed their newborns to neonatal abstinence syndrome (NAS) 6,4. It could be argued that with these statistics, all such pregnant women should be reported for child abuse because the vulnerable unborn child is at an increased risk of harm. It cannot articulate its right to life and should be protected. The argument is that ethical principles should be applied to the unborn foetus as they would to an independent human. However, this is a hard argument to put forward, as the foetus is only a future child because of the incubation of the mother’s body. To make this argument, according to Karpin 7 renders the woman’s body irrelevant and a “complex process of disappearing has to take place”. There is a long held belief that the foetus may be a human in-utero, but only gains personhood at birth 8. In Wilkinson et al.’s 5 counter argument paper about protecting future children, they propose legal actions that could be taken against the mother post-natally for in-utero harm. This could lead to a maternal decision to terminate the pregnancy. In order to avoid harm to the foetus, they also suggest termination as a possible pre-natal intervention, and instating mandatory termination where the pregnant woman has drunk heavily. These statements appear somewhat counter-intuitive to their argument for protection and only highlight the importance of the woman in this situation. Without removing the mother from the equation as Karpin 7 mentions and accepting that the foetus is connected and a part of her body 9, there is a need to ensure her autonomy is respected. Autonomy is defined as the ability to make choices about oneself that are free of any control, interference or limitations from others 10. Moreover is that these choices be morally respected and that all actions are performed with informed consent 11. Informed consent is the assumption that the person knows their choices and can refuse 12. As a HCP, autonomy may conflict with what is considered to be ‘doing the right thing’ or ‘doing no harm’ 13, however these concepts of beneficence and non-maleficence will be addressed later in the argument. Reporting this woman would be a violation of her right to autonomy as it would not be a choice she would be making freely. A woman’s right to fair justice too, is a basic human need 14. This includes the justice to receive unbiased healthcare, to offer her the best opportunity of flourishing and living without offence in society 15. This Natural Law theory also supports the double effect principle where intentionally caring for and not reporting the pregnant woman may have a foreseen outcome of continuing harm to the foetus, but is still seen as morally permissible 16. When considering what is permissible, HCPs are bound by their objective duty of care based on reason and the rules of their profession 17. Midwives are bound by their code to place the interests of the woman before all else, share the decision making and support her right to refuse 18. Along with other human rights of freedom 19, these form part of what can be explained as the theory of Deontology. This theory is based on intellectual moral obligations of right and wrong and the binding duty to uphold them 17. These duties help ground the argument against mandatory reporting and are also supported by legal regulations. The foetus has no legal rights as a child until they are born alive 20 and there are no rules in Australia implementing mandatory reporting for an expectant mother who misuses alcohol or illicit drugs. There is an exception only in Tasmania in conditions where there is a high likelihood of severe neglect and harm to the future infant 21. In situations where an expectant mother is found to be misusing illicit drugs and alcohol, the HCP has the opportunity to ‘do good’ by providing appropriate treatment that will benefit the woman 16. This principle of doing good is known as beneficence 3 and can be used to build a therapeutic relationship based on trust 22. Patients respond more favourably to recommendations when they trust their professional and feel less vulnerable 23. Providing transparency, confidentiality and avoiding harm and abandonment are ways to reduce the feeling of vulnerability in the woman, gain her trust and increase her honesty 24. Barnard 24 also mentions that “[b]ehaviors alone do not give us all the information we need to make accurate judgments” and this increased connection can open opportunities to get to the origin of the misuse. Counselling, support and education are widely supported measures that may ultimately lead to better outcomes for the mother 5 and consequently, the foetus and future child. This way of ethically looking at the overall, ultimate outcome of a situation where the ends justifies the means and where more good will be produced than harm, is called Consequentialism 17. This theory can be applied to the greater community where it can be assessed if reporting the woman would be better for society or not 25. Mandatory reporting would impact others in the mothers’ family, social group and the greater public 26. Depending on the type and level of usage, negative impacts like those of displacement of other family members, legal proceedings, job disruptions, emotional trauma and a greater societal resource expense of reporting management need to be considered. Avoiding these negative impacts can be defined as ‘doing no harm’ which is the principle of non-maleficence 26. The harms of reporting the mother can be weighed against the principle of beneficence to produce a net benefit over harm 27. In this situation maleficent acts on the mother may include being judgemental, patriarchal, stigmatising and removing her autonomy. Should a person be deprived of what they most value, this deprivation is “often worse than the disease we are attempting to cure” 28. While the arguments have been focused on respecting the pregnant woman and acknowledging the duty of care towards her, it is worth still recognising the impact of the situation on the unborn and future child. Even though the foetus has no legal status, it is still significant in a moral sense and worth considering 5,29. Whether an HCP has a legal duty or not, they may still want to think of themselves as ‘doing the right thing’ ethically for the foetus. This principle is known as Virtue Ethics and focuses on the act of enabling human flourishing, in this case the foetus 16,26. This can be done by finding the middle path and avoiding any extremes 17. This has been accomplished in the previous arguments where focussing on the wellbeing of the woman ultimately has the best chance of the un-born child having more favourable outcomes. Clearly then, there is no reason mandatory reporting for child abuse should be a requirement for pregnant women who misuse alcohol or drugs. It has been shown that the abuse is not imposed on a child, but on an unborn foetus and therefore, by definition, the woman herself. Using Childress & Beauchamp’s 10 four principles as an acceptable basis for medical ethics evaluation 13, it was argued that a woman’s autonomy and right to fair justice should be respected and that the HCP has an obligation to respond within their duty of care and legal parameters. However, it was also identified in research that the HCP has a unique opportunity to therapeutically support the woman’s situation through gained trust, to increase her potential for healthier outcomes. By refraining from reporting, no intentional action of harm has been made and the outcomes for both mother, foetus and future child have been improved. References
(1) Australian Institute of Health & Welfare. National Drug Strategy Household Survey 2019: In Brief. 2019, 104. https://doi.org/10.25816/e42p-a447. (2) World Health Orgnization. Lexicon of Alcohol and Drug Terms Published by the World Health Organization. 2006 http://www.who.int/substance_abuse/terminology/who_lexicon/en/ (accessed Sep 7, 2020). (3) Beauchamp, T.; Childress, J. Principles of Biomedical Ethics, 7th ed.; Oxford University Press: New York, 2013. (4) Price, H. R.; Collier, A. C.; Wright, T. E. Screening Pregnant Women and Their Neonates for Illicit Drug Use: Consideration of the Integrated Technical, Medical, Ethical, Legal, and Social Issues. Front. Pharmacol. 2018, 9, 961. https://doi.org/10.3389/fphar.2018.00961. (5) Wilkinson, D.; Skene, L.; De Crespigny, L.; Savulescu, J. Protecting Future Children from In-Utero Harm: Protecting Future Children from In-Utero Harm. Bioethics 2016, 30 (6), 425–432. https://doi.org/10.1111/bioe.12238. (6) Wabuyele, S. L.; Colby, J. E.; McMillin, G. A. Detection of Drug-Exposed Newborns. Ther. Drug Monit. 2018, 40(2), 166–185. https://doi.org/10.1097/FTD.0000000000000485. (7) Karpin, I. The Uncanny Embryos: Legal Limits to the Human and Reproduction Without Women. 2006, 28, 26. (8) Jarvis Thomson, J. A Defense of Abortion. Philos. Public Aff. 1971, 1 (1), 47–66. https://doi.org/10.2307/2265091. (9) Savell, K. The Legal Significance of Birth. Univ. New South Wales Law J. 2006, 29 (2), 200–206. (10) Childress, J.; Beauchamp, T. Principles of Biomedical Ethics, 5th ed.; Oxford University Press, 2001. (11) International Confederation of Midwives. International Code of Ethics for Midwives https://www.internationalmidwives.org/assets/files/general-files/2019/10/eng-international-code-of-ethics-for-midwives.pdf. (12) Frye, A. Holistic Midwifery: A Comprehensive Textbook for Midwives in Homebirth Practice; Labrys Press: Portland, Oregon, USA, 1995. (13) Gillon, R. Defending the Four Principles Approach as a Good Basis for Good Medical Practice and Therefore for Good Medical Ethics. J. Med. Ethics 2015, 41 (1), 111–116. https://doi.org/10.1136/medethics-2014-102282. (14) Johnstone, M.-J. Nursing and Justice as a Basic Human Need: Nursing and Justice as a Basic Human Need. Nurs. Philos. 2011, 12 (1), 34–44. https://doi.org/10.1111/j.1466-769X.2010.00459.x. (15) Ozolins, J. Ethical Principlism. In Foundations of healthcare ethics : theory to practice; Cambridge University Press: Port Melbourne, Vic., 2015. (16) Kerridge, I.; Lowe, M.; Stewart, C. Principle-Based Ethics. In Ethics and law for the health professions; The Federation Press: Leichhardt, NSW, 2013. (17) Ozolins, J.; Grainger, J. Foundations of Healthcare Ethics : Theory to Practice; Cambridge University Press: Port Melbourne, Vic., 2015. (18) Nursing and Midwifery Board of Australia. Code of Conduct for Midwives. Nursing and Midwifery Board of Australia. 2018. (19) United Nations. Universal Declaration of Human Rights https://www.un.org/en/universal-declaration-human-rights/index.html (accessed Aug 29, 2020). (20) Forrester, K.; Griffiths, D. Manipulation of Life. In Essentials of law for health professionals; Elsevier Australia: Chatswood, NSW, 2010. (21) Heyes, N. Mandatory Reporting of Child Abuse and Neglect CFCA Resource Sheet; Australian Institute of Family Studies, 2020; p 10. (22) WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience; World Health Organization, Ed.; World Health Organization: Geneva, 2016. (23) Paulsen, J. E. Ethics of Caring and Professional Roles. Nurs. Ethics 2011, 18 (2), 201–208. https://doi.org/10.1177/0969733010392302. (24) Barnard, D. Vulnerability and Trustworthiness: Polestars of Professionalism in Healthcare. Camb. Q. Healthc. Ethics 2016, 25 (2), 288–300. https://doi.org/10.1017/S0963180115000596. (25) Mandal, J.; Ponnambath, D.; Parija, S. Utilitarian and Deontological Ethics in Medicine. Trop. Parasitol. 2016, 6(1), 5. https://doi.org/10.4103/2229-5070.175024. (26) Freegard, H. Ethics in a Nutshell. In Ethical practice for health professionals; Cengage Learning Australia, 2012. (27) Gillon, R. Medical Ethics: Four Principles plus Attention to Scope. BMJ 1994, 309 (6948), 184. https://doi.org/10.1136/bmj.309.6948.184. (28) Handerson, V. The Nature of Nursing : A Definition and Its Implications for Practice, Research, and Education : Reflections after 25 Years; National League for Nursing Pres: New York, N.Y, 1991. (29) United Nations. Convention on the Rights of the Child https://www.ohchr.org/en/professionalinterest/pages/crc.aspx. |
JoWife, Mum, Doula, Student Midwife, Event Producer, Website Concocter, Cancer Transitioner, Dancer, Circler, Yogi, Organic, Suburban Hippie Archives
May 2022
Categories |
||||||||||||||||||||||
 RSS Feed
RSS Feed

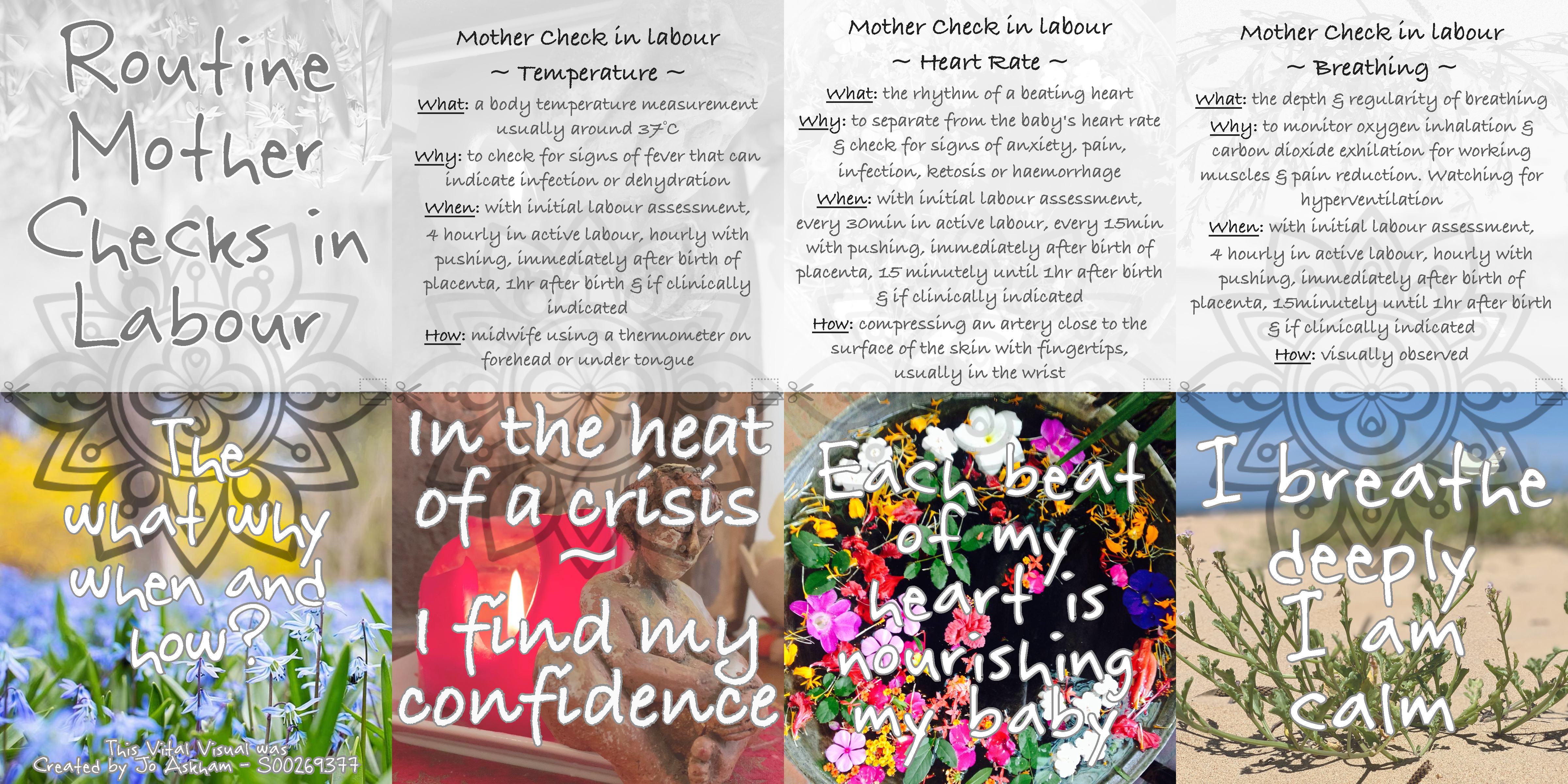{kind=link}
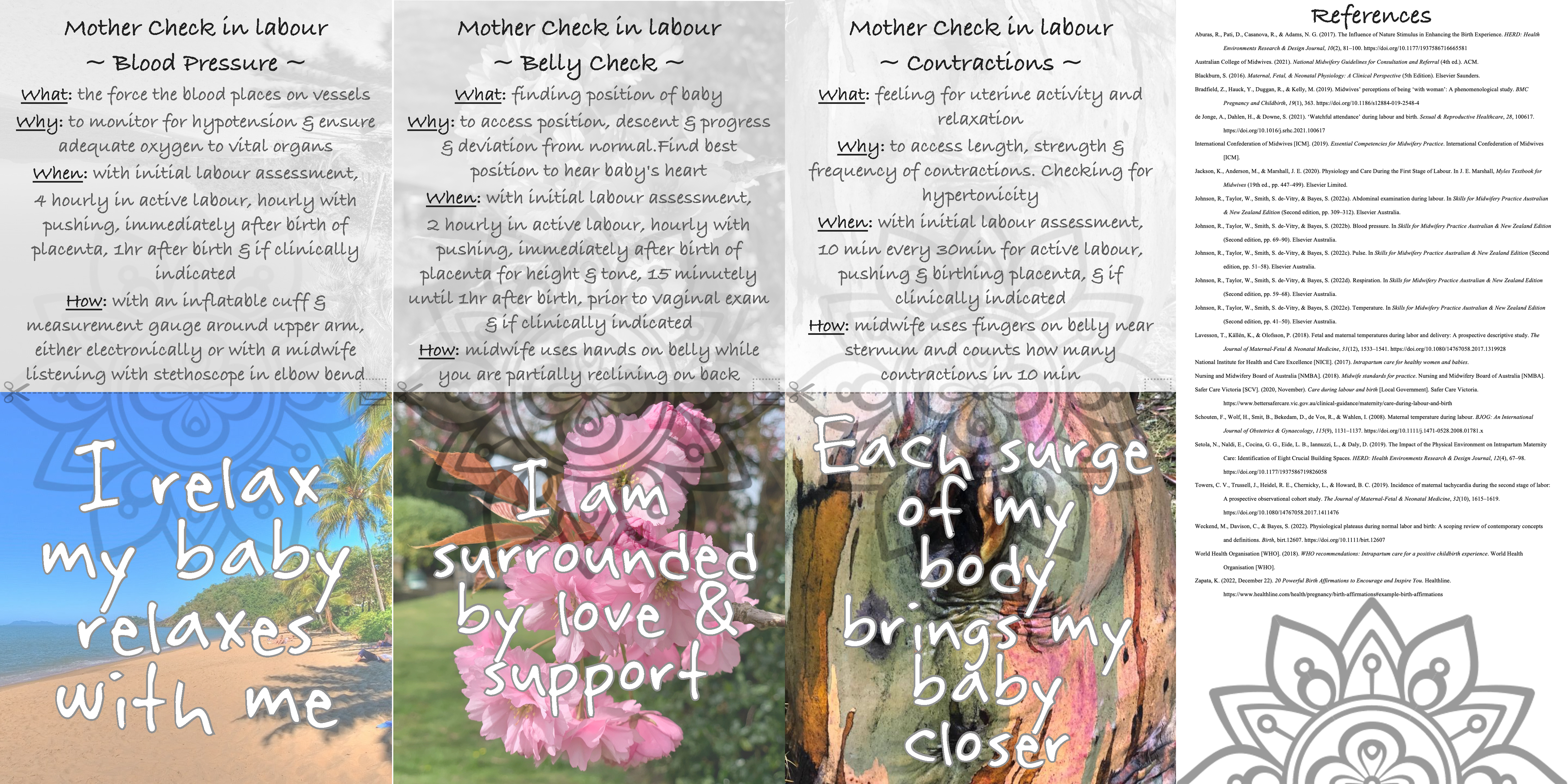{kind=link}